
Approaches to Addressing Serious Mental Illness in the Canadian Criminal Justice System
Press Release
Abstract
Individuals with serious mental illnesses (SMI) are overrepresented in the criminal justice system. Key priorities of the Mental Health Commission of Canada’s National Mental Health Strategy for Canada include reducing the number of people with SMIs involved with the criminal justice system and providing better support to those who are in it. We review promising approaches to addressing SMIs at various junctures within the criminal justice system. In law enforcement, standardized mental health training for officers and specialized response teams have been implemented. The court system has seen the rise of mental health courts that prioritize treatment and rehabilitation. In custody, increasingly accurate mental health screening has become routine, coupled with pharmaceutical and non-pharmaceutical treatments. Promising practices have also emerged in community corrections, including a comprehensive transitional planning model, specialized community supervision for probationers and parolees with SMIs, and methods for improving collaboration across community-based services. More systematic implementation of these practices could reduce the number of criminal-justice involved individuals with SMIs.
Author’s Note
Research Division
Public Safety Canada
340 Laurier Avenue West
Ottawa, Ontario K1A 0P8
Email: PS.CPBResearch-RechercheSPC.SP@ps-sp.gc.ca
Acknowledgements
We would like to thank Dr. Kelly Babchishin, Dr. Amel Loza-Fanous, and Heba Ismail for their input on this document.
Introduction
Everyone experiences fluctuations in the way they feel or how they behave but, for some, these fluctuations interfere with their daily life. According to the American Psychiatric Association, serious mental illness (SMI) refers to a “mental, behavioural, or emotional disorder (excluding developmental and substance use disorders) resulting in serious functional impairment, which substantially interferes with or limits one or more major life activities” (Parekh, 2018, Note, para. 1). Although there is a lack of coherence in the literature regarding which mental illnesses qualify as SMIs, they typically fall under three major categories: psychotic disorders, bi-polar disorders, and major depressive disorders. However, other mental illnesses that cause significant impairment are also commonly considered SMIs, including obsessive-compulsive disorder and post-traumatic stress disorder (PTSD). The current review provides information on the prevalence of individuals with SMIs in Canadian corrections and approaches to addressing mental health in the criminal justice system more broadly. Approaches are organized according to their point of junction with the criminal justice system, including law enforcement, the court system, custody, and the community.
Background
The vast majority of individuals with SMIs do not commit crimes and are non-violent (Mental Health Commission of Canada, 2012) and SMIs are not strong predictors of criminal activity (Bonta & Andrews, 2017; Bonta et al., 1998; 2014;). However, individuals with SMIs are overrepresented in the Canadian criminal justice system (Mental Health Commission of Canada, 2012; Office of the Correctional Investigator, 2015). Contributing to their overrepresentation are numerous social problems that disproportionately affect individuals with SMIs, including poverty, homelessness, unemployment, and low educational achievement (Bonfine et al., 2020). Furthermore, many of the same criminogenic needs that predict criminal recidivism among the general population also predict recidivism among individuals with SMIs (Bonta et al., 2014), but social factors compound these needs in individuals with SMIs (Bonfine et al., 2020).
In 2012, the Mental Health Commission of Canada put forth the National Mental Health Strategy for Canada (NMHSC). Key priorities of this federal, provincial, and territorial strategy are to “reduce the over-representation of people living with mental health problems and illnesses in the criminal justice system, and provide appropriate services, treatment, and supports to those who are in the system” (Mental Health Commission of Canada, 2012, p. 46). Meta-analytic findings suggest that, within high income countries (e.g., Canada), rates of SMIs in prisons have remained relatively stable (Fazel & Seewald, 2012). Consistent with international trends, there has been little change in the rates of SMIs among newly federally sentenced men in Canada over the last 15 years (Beaudette et al., 2015; Brink et al., 2001). Interestingly, however, inmates’ self-reported mental health needs and access to treatment appear to be increasing (Correctional Service Canada, 2009), which may reflect a greater willingness to report symptoms of mental illness and/or greater ability to detect mental illness among this population. Nonetheless, more could certainly be done to address the needs of individuals with SMIs in the criminal justice system.
Prevalence of SMIs
Estimates suggest that mental illnesses are up to three times more prevalent in federal correctional institutions than in the general population (Brink et al., 2001; Office of the Correctional Investigator, 2015). In a Canadian national study of newly admitted men in federal correctional institutions (N = 1,110), 12% met the diagnostic criteria for an SMI (Beaudette & Stewart, 2016). The Atlantic (16%) and Ontario (15%) regions had the highest rates of incoming federal inmates with an SMI, followed by Quebec (13%), the Prairies (10%), and Pacific regions (7%; Beaudette et al., 2015). Among men incarcerated in Canada, estimates suggest that 2-5% have a current psychotic disorder (e.g., schizophrenia; Beaudette & Stewart, 2016; Bland et al., 1998; Brink et al., 2001; Corrado et al., 2000), 6-14% have a major depressive disorder (Beaudette & Stewart, 2016; Bland et al., 1998; Corrado et al., 2000;), 4% have a bipolar disorder (Beaudette & Stewart, 2016; Corrado et al., 2000), and 16% borderline personality disorderFootnote1 (Beaudette & Stewart, 2016).
Estimates suggest that rates of SMIs are slightly higher among newly admitted federally sentenced women (17%; Brown et al., 2018) than men (12%; Beaudette et al., 2015). However, these findings are based on a substantially smaller sample of newly admitted women (N = 86) than men (N = 1,110). When the sample of newly admitted federally sentenced women was combined with a larger in-custody sample (combined N = 246), 5% of women had a current psychotic disorder, 10% had a current major depressive disorder, and 4% had a current bipolar disorder (some disorders were co-occurring). These rates fall within the ranges reported for men above. Furthermore, in a sample of 171 women and 500 men incarcerated in a Quebec provincial jail, women and men had the same rate of schizophrenic disorders (6%); however, women were more frequently diagnosed with depressive disorder (26% for women and 20% for men) and affective psychoses, such as bipolar disorder (13% for women and 7% for men; Lafortune, 2010). Additionally, the proportion of women in federal prison meeting the diagnostic criteria for borderline personality disorder is twofold compared to men (33% [Brown et al., 2018] vs. 16% [Beaudette & Stewart, 2016]). Research also shows that women are more likely than men to be identified as “mentally disordered” (Canadian Public Health Association, 2004, p. S37) or as exhibiting “severe symptoms” of mental illness (Brown et al., 2015, p. 40). Notably, more than twice as many federally sentenced women are diagnosed with current PTSD compared to federally sentenced men (e.g., 27% [Brown et al., 2018] vs. 11% [Beaudette & Stewart, 2016]), possibly because they are more frequently victims of sexual and physical violence (Derkzen et al., 2013; Leschied, 2011).
A Canadian study suggests that older inmates (> 65 years of age) may have a higher prevalence of mental illnesses than younger inmates (Brink et al., 2001). However, research from the United States indicates that rates of SMIs do not significantly differ between younger and older inmates (> 50 years of age; Al-Rousan et al., 2017). More research is needed on the prevalence of SMIs among aging inmates in Canada.
Indigenous persons represent approximately 24% of the federal offender population, but only 5% of the Canadian adult population (Public Safety Canada, 2019; Statistics Canada, 2018). Despite their overrepresentation in the criminal justice system, little research has examined SMIs among criminal justice-involved Indigenous persons in Canada. Among men entering Canadian federal institutions, Indigenous and non-Indigenous inmates had similar rates of current mood disorders (18% for Indigenous and 17% for non-Indigenous), psychotic disorders (2% for Indigenous and 4% for non-Indigenous), and anxiety disorders (32% for Indigenous and 29% for non-Indigenous; Beaudette & Stewart, 2016). Similarly, in a national sample of federally sentenced women, rates of SMIs did not significantly differ between Indigenous (19%) and non-Indigenous women (16%; Brown et al., 2018). It is worth noting, however, that inmates of Indigenous ancestry have higher rates of substance use disorders (Beaudette & Stewart, 2016; Brown et al., 2018), which may exacerbate symptoms of SMIs (e.g., Johns, 2001; Swofford et al., 1996). More research is needed to better understand the prevalence of SMIs among Indigenous persons involved in the Canadian criminal justice system.
There is a dearth of research on the prevalence of SMIs among other racialized groups involved with the criminal justice system. Most studies only include a small number of individuals from other racialized groups, such as those of African-Canadian/American or Asian ancestry, from which rates of SMIs cannot be reliably estimated. Nonetheless, in a Canadian sample of 495 federally sentenced men, racialized groups had an overall lower prevalence of diagnosed mental illnesses causing moderate to severe impairment (13%) compared to White (25%) and Indigenous (23%) inmates (Martin, Wells et al., 2018a). Similarly, another study found that fewer African-American individuals tend to self-report a recent history of mental illness when entering Canadian federal institutions (Martin, Crocker et al., 2018). Research from the United States also suggests that African-American and Latino people are less likely to self-report taking medication or being hospitalized for mental illness prior to entering jail (Prins et al., 2012). More research is needed on the rates of SMIs among criminal justice-involved racialized groups in Canada.
Importantly, most federally sentenced individuals with SMIs also have another concurrent mental disorder. Among newly admitted federally sentenced men with a diagnosed Axis I mental disorder (i.e., psychotic disorders, mood disorders, anxiety disorders, and eating disorders; N = 439), 17% (n = 76) had a concurrent substance use disorder, 17% (n = 76) had a concurrent personality disorder (antisocial personality disorder or borderline personality disorder), and 45% (n = 199) had both concurrent substance use and personality disorders in addition to their Axis I diagnosis (Stewart & Wilton, 2017). That means that only 20% (n = 88) of federally sentenced men with a diagnosed Axis I mental disorder did not have a diagnosed concurrent disorder. Evidence suggests that individuals with concurrent disorders have poorer institutional (e.g., institutional incidents) and community (e.g., recidivism) outcomes (Stewart & Wilton, 2017; Wilton & Stewart, 2017).
Law Enforcement
Individuals with SMIs are more likely to come in contact with law enforcement officers and be arrested for relatively minor offences compared to the general Canadian population (Charette et al., 2014; Hoch et al., 2009). Consequently, one way to reduce the overrepresentation of individuals with SMIs in the criminal justice system is to divert them from the system altogether. Law enforcement officers play an integral role in diverting individuals with SMIs from the criminal justice system as they are typically the first point of contact with the system. Additionally, they are given broad discretion regarding arrest and diversion. Officers have several diversion options, including connecting the individual to community-based mental health services, bringing them home, escorting them to a hospital emergency department, and referring them to a local diversion program (e.g., ConnexOntario Pre-Charge Diversion program; ConnexOntario, 2019). It is essential that officers receive sufficient mental health training to help them make appropriate decisions regarding diversion.
In Canada, all new law enforcement recruits receive at least some form of mental health training; however, past research has shown that the length of training varies across organizations ranging from one to 24 hours (Cotton & Coleman, 2008). Furthermore, this level of training may be insufficient. The Mental Health Commission of Canada (2012) has proposed that new law enforcement officers should receive approximately 35 to 40 hours of training on mental illness to build the knowledge and skills required to effectively interact with this population. The Commission also put forth the Training and Education about Mental Illness for Police Organizations (TEMPO) framework to help law enforcement organizations develop and assess their mental health training programs (Coleman & Cotton, 2014). Within this framework, several recommendations are made, such as including individuals with SMIs in the development and administration of training modules to help decrease stigma, placing a greater focus on communication skills and de-escalation techniques, and incorporating an evaluation component that the officers must pass prior to deployment. This framework is the first step towards a more standardized approach to mental health training for law enforcement officers in Canada.
One promising training program, the Crisis Intervention and De-escalation (CID) Training, was implemented in British Columbia (BC; Coleman & Cotton, 2014). Since January 2012, all new recruits are required to complete the training, including RCMP officers. The CID Training consists of a 3-4 hour online course and seven hours of in-class learning, followed by role plays conducted within individual police agencies. The course covers SMIs and related symptoms, situational risk assessment, de-escalation techniques, and the BC Mental Health Act. Law enforcement officers in BC must also participate in the mandatory requalification training section of the program every three years. If an adequate learning module is not already in place, law enforcement agencies could consider modeling their crisis intervention and de-escalation training after the CID training program. This type of program could also be supplemented by additional training as recommended in the TEMPO framework (Coleman & Cotton, 2014).
In addition to mental health training, specialized response teams have been initiated in some regions across Canada to improve responses to crisis situations involving individuals with SMIs. These teams typically include a co-response by specially trained law enforcement officers and mental health professionals (e.g., nurses) at the request of the first responding officers (Shapiro et al., 2015). The idea behind the co-response model is that mental health professionals can provide mental health consultations and service referrals, while law enforcement officers can ensure the safety of all persons involved. One example of a specialized co-response team is the Crisis Outreach and Support Team (COAST) in Hamilton (COAST Hamilton, n.d.). COAST provides services to residents of the city of Hamilton who have serious mental health issues and are in crisis. Crisis Triage and Support Workers answer calls on the COAST crisis line, they assess situations, and provide recommendations for services and treatment. There is also a mobile outreach team that consists of one plain-clothed officer and one mental health professional who visit individuals with SMIs in the community to complete assessments, develop response plans, and conduct follow-ups. The use of specialized co-response teams has been associated with lower arrest rates, increased referrals to community mental health services, and reduced time spent responding to crisis situations or waiting in the emergency room with the person in crisis (e.g., Koziarski, 2018; Shapiro et al., 2015). Cost-benefit analyses conducted outside of Canada have also found that co-response teams can be cost-effective. For example, Scott (2000) found that a co-response team in the United States resulted in a 23% reduction in costs per case compared to the typical law enforcement response. Despite the various advantages of co-response programs, however, the lack of resources allocated to these teams results in very low response rates. For instance, in Ontario, most police co-response teams respond to less than 25% of crisis situations (Durbin et al., 2010). Additionally, most co-response teams are not available 24 hours a day, which limits their usefulness. It is important that future research continues to evaluate the co-response model in Canada to determine if these programs warrant additional funding.
Another type of initiative that responds to the needs of individuals with SMIs is known as a Hub Model, such as the one in Alberta’s Samson Cree Nation. This model is a risk-driven intervention designed to reduce crime by facilitating information sharing across sectors (e.g., police, probation, mental health, harm reduction, outreach; Nilson, 2016). Representatives from each sector meet regularly to discuss high-risk cases and develop support strategies for these individuals. If research demonstrates the effectiveness of this model in managing high-risk clients, other communities could consider its implementation.
Another promising practice that has emerged in Canada is the use of the interRAI Brief Mental Health Screener (BMHS), a mental health screening tool developed to help law enforcement officers recognize indicators of SMIs and to communicate their observations to mental health professionals (Hoffman et al., 2016). The interRAI BMHS is currently being used by the Ontario Provincial Police and about 45 other police services across Ontario, Manitoba, Saskatchewan, and British Columbia (interRAI Board Member, personal communication, August 27, 2019). In a pilot study, police officers in Wellington, Ontario were trained to complete the interRAI BMHS (Hoffman et al., 2016). When officers decided to bring an individual to the hospital, they would provide the emergency department staff with a copy of their assessment. Results of the pilot study suggest that police primarily brought individuals to the hospital because of their potential for violence (e.g., self-harm or harm against other), while emergency department staff tended to admit individuals who exhibited disordered thought and psychosis. These results could be used to help align the goals of law enforcement and mental health professionals in order to reduce unnecessary visits to the emergency department. Future research could also examine the benefits of using mental health screening tools for improving communication between law enforcement officers and mental health staff, and the extent to which such tools can help officers decide whether to bring an individual to the hospital.
Court System
There are two main provisions in the Canadian criminal code that may apply to individuals with SMIs who have been charged with a criminal offence: unfit to stand trial and not criminally responsible on account of mental disorder (NCRMD). Fitness to stand trial is based on the person’s ability to understand the nature of the proceedings and the various legal consequences they face, communicate with their lawyer, and ultimately participate in their own defense. The presiding court may order an assessment of the accused’s mental condition if there are reasonable grounds to believe that the accused may be unfit to stand trial (Criminal Code, R.S.C., 1985, s 672.11 (a)). If a person is found unfit to stand trial, they would receive treatment for their mental illness at a forensic hospital until they are found to be fit, after which legal proceedings may resume. Briefly, forensic hospitals are responsible for conducting court ordered assessments (e.g., fitness to stand trial) and providing treatment to individuals who are found unfit to stand trial or NCRMD. A person may be found NCRMD if it is determined that the they were incapable of understanding the nature of their actions or were unaware of the wrongfulness of their actions during the commission of the offence (Criminal Code, R.S.C., 1985, s 16 (1)). If a person is found NCRMD, they may receive an absolute discharge, a conditional discharge (e.g., required to attend mental health treatment), or detention in a forensic hospital.
Importantly, NCRMD verdicts are rare. In fiscal year 2011/12, Québec only recorded 540 new verdicts of NCRMD (Crocker et al., 2015). Similarly, in Ontario, only 170 new cases of NCRMD were recorded in the year 2010/11 (Crocker et al., 2015). Given that the majority of accused individuals with SMIs are eventually fit to stand trial and do not meet the strict criteria for NCRMD, it is important to consider approaches to addressing the needs of this population within the criminal court system. One promising approach involves specialized courts, such as mental health courts. Mental health courts were created in response to the high rates of mental illness in the criminal justice system and are designed to better address the needs of individuals with SMIs. They are typically less formal, composed of a multidisciplinary team of judges, lawyers, and mental health professionals, and offer diversion programs that provide an alternative to criminal sanctions (Schneider, 2010).
Eligibility criteria can vary widely across mental health courts. For instance, some mental health courts require full acceptance of responsibility under the law before participation is permitted while others do not (Slinger & Roesch, 2010). Additionally, several courts only accept individuals who have committed minor summary offences while others will accept those accused of summary or indictable offences. Notably, few mental health courts accept individuals accused of violent offences. However, research shows that individuals accused of violent and felony offences (equivalent to indictable offences in Canada) who participated in a mental health court were less likely to reoffend than non-participants one year following their index offence (Anestis & Carbonell, 2014). Mental health courts could therefore consider the possibility of expanding their eligibility criteria to include a wider range of individuals.
The types of diversion programs offered by mental health courts also vary. In general, however, they involve complying with community-based treatment and programming requirements. Most Canadian mental health courts will use informal rather than criminal sanctions if compliance is not maintained, such as increasing the number of required court appearances (Slinger & Roesch, 2010). If the program is successfully completed, these courts will typically drop the criminal charges, diverting successful participants out of the criminal justice system without any new charges. In addition to diverting individuals with SMIs from the criminal justice system, diversion programs aim to reduce the likelihood of reoffending. Therefore, it is important that diversion programs also address criminogenic needs (e.g., pro-criminal attitudes) in addition to symptoms of mental illness to reduce repeated involvement with the criminal justice system (Bonta et al., 1998; 2014).
Despite the rapid expansion of mental health courts in Canada, surprisingly little empirical research has examined their effectiveness (Slinger & Roesch, 2010). To date, one study showed that program participants spent significantly fewer days in custody per month after starting a mental health court program compared to before; although this study did not include a control group (Watts & Weinrath, 2017). A study of 708 individuals diverted to one of five mental health courts in Toronto found that approximately two-thirds of program participants successfully completed the program (Seto et al., 2018). Older individuals with a lower number of clinical needs and fewer prior offences were more likely to successfully complete the program (Seto et al., 2018), suggesting that it is important to tailor programs to the needs and characteristics of individual clients.
While there is a dearth of research on mental health courts in Canada, they have received more empirical attention in the United States. A synthesis of this research suggests that mental health courts are associated with moderately lower rates of reoffending (standardized mean difference = -.54; Sarteschi et al., 2011); however, evidence for their relation to clinical outcomes is mixed (Honegger, 2015). A multi-site, longitudinal evaluation of mental health courts in the United States also found that, after an 18-month follow-up period, mental health court participants were less likely to be arrested than non-participants (49% vs. 58%; Steadman et al., 2011). More Canadian research is needed to understand the short- and long-term benefits of mental health courts across Canada and, specifically, among women and racialized groups. Additionally, their impact on clinical outcomes, such as symptoms of SMIs, needs to be examined more rigorously.
Custody
Despite efforts to divert individuals with SMIs out of the criminal justice system, a large number still end up in correctional institutions. In 2012, a Mental Health Strategy for Corrections in Canada was developed with the goal of better serving the needs of individuals with SMIs in the federal correctional system (Correctional Service Canada, 2012a). It aims to provide timely access to mental health services in custody and improve continuity of care. Guiding principles also include equal access to mental health care for all individuals in the correctional system, client-centered, culturally-sensitive, and gender-appropriate mental health services, and the promotion of mental well-being. Screening, assessment, and treatment form the basis of correctional mental health models aimed at addressing the needs of inmates with SMIs.
Screening and assessment
Mental health screening and assessment is essential in identifying and providing treatment to individuals with SMIs. Screening tools used in provincial facilities include the Brief Jail Mental Health Screen (BJMHS) and the Jail Screening Assessment Tool (JSAT; see Martin, Colman et al., 2013a for a review). In general, both tools correctly screen in over 60% of individuals with SMIs and correctly screen out over 65% of individuals who do not have a SMI (Martin, Colman et al., 2013b). In federal institutions, Correctional Service Canada uses the Computerized Mental Health Intake Screening System (CoMHISS; Correctional Service Canada, 2018). CoMHISS is a computerized questionnaire that includes measures of mental health history, self-harm, and psychological distress (i.e., Brief Symptom Inventory [Derogatis, 1993] and Depression, Hopelessness and Suicide Screening Form [Mills & Kroner, 2004]). It takes about 45 minutes to complete and is typically administered within 14 days of arrival at the institution (Martin, Wamboldt et al., 2013). Anyone who self-reports a history of mental health issues or endorses any of the self-harm risk questions is flagged for further assessment with a mental health professional (Correctional Service Canada, 2018). Additionally, anyone who exceeds the cut-off scores on the Brief Symptom Inventory or the Depression, Hopelessness and Suicide Screening Form is flagged for further file review and, based on clinical judgment, may be referred for an in-person assessment with a mental health professional. This screening method correctly screens in 75% of inmates with SMIs and correctly screens out 71% of inmates without SMIs (Martin, Wells, et al., 2018a).
It is important to note that screening tools are only a first step in identifying individuals with SMIs and are therefore over inclusive. For example, on average, CoMHISS screens in 29% of inmates who are not mentally ill or have low mental health needs (Martin, Wells, et al., 2018a). Therefore, further assessment is required for those who are screened in by mental health screening tools to ensure the most efficient use of mental health resources. Evidence suggests that screening tools may be less effective at identifying SMIs among women, Indigenous people, and other racialized groups (Martin, Coleman, et al., 2013a; Martin, Wells, et al., 2018a). It is important that research continues to examine the generalizability of these tools to all justice-involved individuals and, if required, develop appropriate measures.
In 2014, 27% (n = 1,081/3,983) of federal offenders screened using CoMHISS were flagged for further assessment (Delveaux et al., 2017). Among those flagged by CoMHISS, 95% received a follow-up service within CSC’s guidelines at the time of 50 days from admission or 40 days from referral. However, a lack of human resources (e.g., psychologists, forensic nurses) in some institutions may limit timely access to mental health services (e.g., Canada, Parliament, Senate. Standing Senate Committee on Human Rights, 2019; Office of the Correctional Investigator, 2013). One promising approach for facilitating access to mental health assessments and services, especially in remote locations, is the use of telecommunication to connect inmates to psychologists, psychiatrists, or forensic nurses who are located in other regions (Desai et al., 2013; Ferrazzi & Krupa, 2018). Evidence suggests that the use of telecommunication for delivering psychiatric services can be reliable, beneficial, and cost-effective in forensic settings (Deslich et al., 2013; Sales et al., 2018).
Given high rates of concurrent disorders among criminal-justice involved individuals, it is also important that screening processes can identify concurrent disorders, such as concurrent SMIs and substance use disorders, in order to provide appropriate mental health services (McKee, 2017). Furthermore, it is important that mechanisms are in place to ensure ongoing evaluation and observation of behavioural indicators of mental illness throughout an inmate’s sentence (Livingston, 2009). Correctional officers are in a unique position to be able to identify and monitor symptoms of mental illness because they have the most contact with the inmates. Therefore, providing mental health training to all correctional officers and staff who work closely with inmates could help them recognize and respond to signs of mental illness (Livingston, 2009). Effective communication between correctional officers and mental health staff can facilitate the diagnosis and management of inmates with SMIs (Appelbaum et al., 2001).
Treatment
Provincial and territorial governments are responsible for providing mental health care to individuals serving a sentence of less than two years or who are awaiting trial; whereas, Correctional Service Canada is responsible for providing mental health care to individuals sentenced to two years or more. Minimum standards of care suggest that inmates should receive the same level and standard of care in jail or prison as is available to individuals in the community (Correctional Service Canada, 2012a; Livingston, 2009). Additionally, inmates living with a mental illness should have access to a continuum of services that match their level of need. Correctional mental health treatment generally falls within two main categories: pharmaceutical and non-pharmaceutical treatment.
Pharmaceutical treatment
In a study on psychotropic medication use among incarcerated federal offenders, regional pharmacists across Canada provided a single-day snapshot (September 29, 2014) of all active prescriptions (Farrell Macdonald et al., 2015). Thirty percent of the federal inmate population was identified as having an active prescription, which is approximately four times higher than the general population (8%; Farrell Macdonald et al., 2015). This is consistent with the higher rates of SMIs observed in correctional populations relative to the general population. There were no differences across Indigenous and non-Indigenous inmates, but more women than men had an active prescription (46% vs. 30%). Additionally, some inmates were taking multiple types of medications to treat their mental illness(es). Medications with antidepressant properties were the most commonly prescribed (23%), followed by those with antipsychotic properties (10%), anxiety/insomnia medication (6%), central nervous system (CNS) stimulants (4%), and medication with antimanic agents (less than 1%; Farrell Macdonald et al., 2015).
Despite the substantial proportion of inmates who are prescribed psychotropic medication, there is little research on its effectiveness for improving symptoms of SMIs in prison or jail settings (Barnao & Ward, 2015; Fazel et al., 2016). There is evidence, however, that antipsychotic medication may reduce violence in forensic settings (Barnao & Ward, 2015). Additionally, in a study of criminal-justice-involved individuals diagnosed with schizophrenia in BC (N = 11,462), high adherence (medication possession ratioFootnote2 greater than 80%) to antipsychotic medication was associated with significantly lower rates of violent and non-violent recidivism (up to 128% and 65% lower, respectively; Rezansoff et al., 2017). Similarly, in a Swedish cohort study, having an active prescription for antipsychotic or psychostimulant medication was associated with less violent reoffending after release from prison; however, having an active prescription for antidepressants was not associated with violent offending (Chang et al., 2016). More research is needed to understand the impacts of psychotropic medication on different outcomes among inmates, such as symptom relief and institutional behaviour.
Non-pharmaceutical treatment
A review of 37 studies on non-pharmaceutical therapies administered in custody found that these treatments were associated with improved mental health outcomes, such as decreased depression, anxiety, and overall psychopathology (average d = 0.50, 95% CI [0.34, 0.66], k = 37; Yoon et al., 2017). However, these improvements were not statistically significant at 3-month (d = 0.29, 95% CI [-0.05, 0.64], k = 6) or 6-month follow-ups (d = 0.06, 95% CI [-0.15, 0.26], k = 5; Yoon et al., 2017). Treatment outcomes did not significantly differ between group and individual therapies, suggesting group therapy may be more cost-effective (Yoon et al., 2017). Research also tends to support the use of an open-admission policy rather than a closed-admission policyFootnote3, as well as the use of homework and behavioural practice components in treatment (Morgan et al., 2012). There is no clear consensus regarding which treatment programs are the most effective; however, those that are based on cognitive-behavioural therapy (CBT; see the Appendix for a description) have shown promise in reducing psychological distress and changing dysfunctional thinking (Knabb et al., 2011). Examples of specific institution- and community-based non-pharmaceutical treatment approaches for individuals with mental illnesses are provided in the Appendix.
In a national study of Canadian federal institutions, inmates were 9% less likely to be involved in an institutional incident, 30% less likely to receive an institutional charge for a serious offence, and 32% less likely to be involuntarily segregated after receiving non-pharmaceutical mental health treatment relative to before they received treatment (Delveaux et al., 2017). Inmates who received treatment were also 23% more likely to complete a correctional program and 34% more likely to complete an educational course compared to before treatment. In another study of federal inmates, compared to pre-treatment, being in treatment was non-significantly associated with lower rates of institutional health incidents (i.e., self-injury, attempted suicide, overdose, or death) among individuals first flagged by the institution’s mental health screening tool as potentially having a mental illness, and rates continued to decline after treatment (Martin, Wells et al., 2018b). In contrast, among individuals with a known mental illness (e.g., official record of mental illness), treatment was non-significantly associated with increased risk of a first institutional health incident but significantly associated with reduced risk of repeated health incidents; post-treatment risk tended toward pre-treatment rates. Additionally, for all inmates, receiving treatment was significantly associated with fewer violent (i.e., instigator of fight, assault, or murder) and victimization (i.e., victim of violent incident) incidents compared to pre-treatment, with violent and victimization incident rates trending toward pre-treatment rates once the inmate stopped receiving treatment.
After release, mental health treatment alone has not consistently been linked to lower rates of reoffending (Morgan et al., 2012). Recall that SMIs are not strong predictors of criminal behaviour, but rather, many of the same criminogenic needs (e.g., pro-criminal attitudes, antisocial associated, substance abuse) predict criminal behaviour for individuals with and without SMIs (Bonta & Andrews, 2017; Bonta et al., 2014). Therefore, addressing symptoms of mental illness may be necessary but not sufficient for reducing criminal reoffending (Skeem et al., 2015). The literature suggests that it is important that correctional programs target individuals who are at medium and high risk to re-offend and address their criminogenic needs in a way that is sensitive to individual/environmental characteristics, mostly using CBT, in order to reduce criminal recidivism. This is known as the risk, need, and responsivity framework (Andrews et al., 1990; Bonta & Andrews, 2017). Within this framework, SMIs are sometimes considered specific responsivity factors that may need to be addressed before or concurrently so that an individual can benefit from correctional programming (Skeem et al., 2011; 2015). For example, symptoms of psychosis would likely need to be treated before one can participate fully in correctional programming. For concurrent SMIs and substance use disorders, however, best-practice is to provide integrated treatment, such that the SMI and substance use disorder are treated at the same time (Canadian Centre on Substance Abuse, 2009). Given that substance use is a criminogenic risk factor (Bonta & Andrews, 2017), integrated treatment represents an opportunity to address symptoms of mental illness and risk of recidivism.
Provision of Mental Health Services
Correctional Service Canada currently offers three different levels of mental health care: primary, intermediate, and intensive care (Correctional Service Canada, 2012b). Primary care involves early mental health assessment and intervention as well as referrals to higher levels of care. Intermediate mental health care is divided into moderate and high intensity care and provides assessment, treatment, and symptom management to inmates who require a higher level of care but do not require hospitalization. Intensive care is provided at regional treatment centres for inmates with acute mental health concerns.
Intermediate care was implemented in 2015 to fill the gap in service between primary and intensive care (Delveaux et al., 2017). To accomplish this, psychiatric hospital beds in regional treatment facilities were de-listed and turned into intermediate care beds. However, the Office of the Correctional Investigator (2015) cautions that more intermediate and intensive care beds may be required to meet the needs of individuals with SMIs in federal correctional institutions. One option to increase treatment capacity would be to increase the use of section 29 of the Corrections and Conditional Release Act (CCRA). This section of the CCRA allows an inmate to be transferred to a community hospital, including any mental health facility, to receive treatment. In many cases, community hospitals may be better equipped to provide mental health services to individuals with SMIs. However, it appears that section 29 of the CCRA is rarely utilized (Canada, Parliament, Senate. Standing Senate Committee on Human Rights, 2019)
Health care delivery models are less concrete across provincial and territorial correctional facilities, but it is important that each region has a model of correctional health care that is consistent with the Mental Health Strategy for Corrections in Canada. British Columbia, for example, has implemented a model of care that focuses on the needs of inmates with complex medical, mental health, and substance use issues, while also considering the unique needs of women, Indigenous, aging, and transgendered people (BC Mental Health and Substance Use Services, 2017). British Columbia was also one of the first provinces in Canada to reassign the Justice Ministry’s correctional health care responsibilities to the Health Ministry (BC Mental Health and Substance Use Services, 2019). This decision was in response to recommendations by the College of Family Physicians of Canada and the World Health Organization.
Best-practice guidelines suggest that inmates with the greatest mental health needs should receive the highest intensity treatment, whereas, those with more basic needs should receive no or low intensity treatment (Livingston, 2009). However, this is not necessarily the case in practice. For instance, a study of Canadian federal inmates found that 69% of inmates who received treatment did not meet the diagnostic criteria for a mental illness, and only 46% of inmates who met the diagnostic criteria received treatment relatively regularlyFootnote4 (Martin, Potter et al., 2018). This suggests that a large proportion of resources is being allocated to inmates with low mental health needs, leaving fewer resources to address the needs of those with SMIs. Other factors that may be associated with the likelihood of receiving mental health treatment include gender, ethnicity, and geographic region (Martin, Crocker et al., 2018). Men and non-Indigenous racialized groups, for instance, were found to have lower rates of mental health treatment regardless of their self-reported mental health needs (Martin, Crocker et al., 2018). Additionally, Atlantic Canada, Québec, and Pacific regions had higher rates of inmates reporting mental health needs upon screening who did not receive treatment relative to other regions (Martin, Crocker et al., 2018). It is possible that discrepancies between screening results and treatment reflect false positives (i.e., individuals without mental health needs who are screened in by the screening tool as potentially requiring mental health treatment). Furthermore, evidence suggests that some inmates with mental health needs may refuse treatment for various reasons (Morgan et al., 2007). In a study of two London prisons, up to 10% of inmates refused treatment for their mental health needs (Jakobowitz et al., 2017). Research on reasons for treatment refusal and treatment termination (in particular among sub-groups with lower levels of access such as men and non-Indigenous racialized groups) could highlight areas for improvement in the delivery of institutional mental health services.
Of note, individuals with SMIs (especially those with concurrent personality and/or substance use disorders) have historically been overrepresented in administrative segregation, a type of confinement for inmates who cannot be managed safely in the general inmate population (Office of the Correctional Investigator, 2015; Stewart & Wilton, 2017). Long-term segregation has been linked to worsening mental health symptoms, including self-harm and suicide (Correctional Service Canada, 2013; Office of the Correctional Investigator, 2015). In 2019, the use of segregation was eliminated in federal institutions and replaced with Structured Intervention Units (SIU; Bill C-83: An Act to amend the Corrections and Conditional Release Act and another Act, 2019). Like administrative segregation, an inmate may be transferred to an SIU when they cannot be safely managed in the general population; however, SIUs are designed to address the individual needs of inmates, including those with SMIs. Legislation outlining the use of SIUs includes mental health assessments, a minimum of four hours outside of the inmate’s cell and two hours of meaningful human contact every day, and greater oversight in transfer decisions. It also allows health staff to recommend modifying conditions of confinement or removing the inmate from the SIU for health reasons. Additionally, inmates living in SIUs have access to treatment and programming that address their needs. Evidence regarding the outcomes of SIUs on inmates’ mental health is not yet available, although this represents an important area for future research.
Community Corrections
Community corrections consist of various activities, the primary ones being transitional planning, community supervision, and community-based services. It is important that mental health needs are considered within each of these activities. Minimum standards require that criminal justice-involved people living with a mental illness receive the same level of mental health care in the community as the general population, that they undergo continuous mental health evaluation, and receive timely access to mental health services (Livingston, 2009).
Transitional planning
Transitional planning—also known as discharge or release planning—is essential for the successful community reintegration of people involved with the criminal justice system, particularly for those with SMIs. Ideally, transitional planning would, at a minimum, include the identification of appropriate and available community mental health services prior to release, referrals to those services, and the management of medication to ensure people have a sufficient supply upon release (Livingston, 2009). Osher et al. (2003) developed a “best-practice” model to guide the transitional planning process called Assess, Plan, Identify, and Coordinate (APIC). The assessment phase involves using validated standardized tools to assess an inmate’s clinical and social needs. The planning phase involves formulating a plan to address short-term and long-term needs through discussion with, and input from, the inmate. It is important that planning begins as soon as an inmate is identified as having a mental illness, especially in jails where incarceration periods are much shorter (Livingston, 2009). The identification phase requires the identification of specific community-based services that meet the client’s needs. Finally, the coordination phase involves executing the plan. Osher et al. (2003) suggest that a specific pre-release coordinator be assigned to each client to improve continuity of care.
One major barrier to achieving continuity of care is that many inmates are released from custody without a health card. Federal inmates do not retain their provincial health care benefits during incarceration; as such, it is the responsibility of institutional parole officers to assist them in obtaining a provincial health card before being released (Delveaux et al., 2017). In response to a survey, 51% (n = 90) of Correctional Service of Canada staff reported issues with this process (Delveaux et al., 2017). For instance, many inmates do not have the documentation required to apply for a health card and cannot afford to obtain the proper documentation. Additionally, some provinces do not allow inmates to apply for a health card until they are released. Two studies in the United States found that inmates who received transitional planning with health care benefit application assistance used more mental health services during re-entry and used them sooner than those who did not receive application assistance (Fontanarosa et al., 2013). Furthermore, receiving mental health treatment upon community re-entry has been associated with lower re-incarceration rates (e.g., Mann et al., 2011). It is therefore important that policies and procedures facilitate the process for obtaining health cards for inmates before release. For example, guidelines could be developed to support the retention of peoples’ health cards during incarceration (Delveaux et al., 2017). This would increase their access to health care upon release and potentially save resources as parole officers would no longer need to facilitate the issuance of new cards. In the meantime, smaller-scale programs, such as Pharmacare in BC, allow criminal justice-involved individuals to access their medication without a health card (Desai et al., 2013).
Community supervision
Most people who receive a sentence for a criminal offence will be under community supervision at some point during their sentence; they may be sentenced to probation (i.e., a sentence served in the community) or released on parole after serving part of their sentence in custody. It is important that community supervision officers receive mental health training to help them identify and respond to symptoms of mental illness (Livingston, 2009). Individuals with SMIs are more likely to have their community sentence revoked for technical violations (e.g., breach of conditions of parole) than those without an SMI (Skeem et al., 2014). Notably, Stewart et al. (2018) found that federally sentenced individuals with concurrent SMIs and substance use disorders were the most likely to have their community sentence revoke, whereas those with an SMI alone did not differ from individuals without any mental illnesses. Therefore, it is important for community supervision officers to screen their clients for SMIs and concurrent disorders, such as substance use disorders (IACFP Practice Standards Committee, 2010; McKee, 2017). Identifying probationers and parolees who have SMIs and concurrent disorders is important, as they may require specialized treatment.
Best-practice guidelines encourage community supervision officers to use alternative sanctions in response to minor conditional violations to reduce the overrepresentation of individuals with SMIs in correctional institutions (Livingston, 2009). Indeed, “negative compliance strategies”, such as threats of incarceration, have been found to predict more technical violations among clients with mental illnesses (Manchak et al., 2014). Alternatively, incentives can be used to encourage good behaviour and increased monitoring can be used to discourage bad behaviour. Other promising practices include “firm but fair” officer-client relationships that are characterized by caring, fairness, trust, and an authoritative (rather than authoritarian) communication style (Prins & Draper, 2009, p. vii). Additionally, problem-solving strategies can be used with the client to address issues of compliance and active coordination between the officer and other service providers can increase service utilization (Prins & Draper, 2009).
Specialized community supervision models have been developed to better serve the needs of criminal justice-involved individuals with SMIs. Two such models include Forensic Assertive Community Treatment (FACT) and Forensic Intensive Case Management (FICM; Skeem et al., 2011). FACT involves a multidisciplinary team of specially-trained community supervision officers and mental health professionals, as well as low staff-to-client ratios, client-centered services, and full-time staff availability (Livingston, 2009). FICM is a less resource-intensive alternative that involves specially trained probation and parole officers who connect clients to community-based mental health services, but does not include a multidisciplinary team or full-time staff availability (Skeem et al., 2011). The few studies that have evaluated FACT and FICM models report mixed findings (Epperson et al., 2014; Skeem et al., 2011). One randomized clinical trial found that FACT participants had fewer jail bookings, more contact with community-based services, and spent fewer days in the hospital than those receiving community supervision as usual (Cusack et al., 2010). Despite these positive findings, there is little evidence showing that specialized supervision models improve mental health or criminal justice outcomes (Skeem et al., 2011). Research could explore whether evidence-based community supervision models, such as the Strategic Training Initiative in Community Supervision (STICS; Bonta et al., 2011; in press), are effective for reducing risk of recidivism among criminal justice-involved individuals with SMIs.
Community-based services
It is important that criminal justice-involved individuals with SMIs have access to community-based mental health services. Other important services also include housing, employment, and correctional programming. Receiving mental health services in the community has been associated with lower re-arrest rates among individuals with SMIs (Constantine et al., 2012). One promising initiative that attempts to facilitate access to community-based mental health services is the Community Mental Health Initiative for federal offenders with SMIs (CMHI; Farrell MacDonald et al., 2014). This initiative includes community mental health specialist services, such as clinical social workers, mental health nurses, mental health interventions, and specialized assessments. Community-based residential facilities that received mental health services from CMHI reported having access to psychologists, social workers, and nurses, as well as having good working relationships with these staff (Desai, 2010). Research also shows that men and woman who received community mental health specialist services were less likely to re-offend than those who did not receive these services (Farrell MacDonald et al., 2014).
One of the most important concerns among community-based residential facilities across Canada is the lack of information sharing between service providers (Desai, 2010). Privacy laws and policies designed to protect the privacy of health information often prevent diagnoses and treatment plans from being shared between agencies. This interferes with continuity of care and leads to the duplication of efforts (e.g., multiple psychological assessments). To mitigate these issues, some organizations proactively ask their clients to sign a consent-to-release information waiver to facilitate sharing of information between the service providers who are involved in their care. In the future, agreements can be put in place to improve information sharing and collaboration across services. As an example, the province of Ontario created the Provincial Human Services and Justice Coordination Committee to improve coordination and collaboration among various correctional and community organizations (Human Services and Justice Coordinating Committee, 1997).
Another issue affecting community-based mental health care is the shortage of mental health resources in the community (e.g., psychiatrists, psychologists, mental health nurses; Desai, 2010; Simpson et al., 2013). Some have argued that the lack of resources is due to the deinstitutionalization movement of the 20th century. That is, the money saved from closing psychiatric hospitals during this period was not reinvested in community mental health services (Schneider, 2010). Insufficient resources have led to problems, such as long wait-times for mental health care (e.g., more than one month; Desai, 2010) and difficulties accommodating those with more complex needs. For example, service providers frequently turn away clients with co-occurring mental illness and substance abuse problems. This represents a significant barrier as more than half of those with SMIs have co-occurring substance abuse issues (Beaudette & Stewart, 2016). Organizations that link criminal justice-involved individuals to mental health services in the community have also expressed that exclusionary criteria often prevent individuals with a criminal history or a history of violence from accessing mental health services (Desai, 2010). These (often informal) exclusionary criteria likely exist because mental health service providers do not have the funding to accommodate violent individuals, do not feel comfortable providing services to this population, and are not adequately trained or equipped to address the needs of this population safely. There are currently very few facilities designed to accommodate both safety and mental health needs. The Secure Treatment Unit located in Brockville, Ontario is one of the only facilities of its kind in Canada (Royal Ottawa Mental Health Care Group, n.d.). This 100-bed facility is a hybrid correctional and mental health facility that services 30 provincial correctional centres across Ontario. It was specifically designed to provide secure forensic assessment, treatment, and discharge planning to men who have been diagnosed with mental illnesses. Building more secure treatment units would help accommodate the needs of criminal justice-involved individuals with SMIs who require a higher level of security than can be met in the community. These secure treatment centres could also incorporate gender and culturally informed treatments.
Conclusion
Many promising practices have been implemented to improve the care of individuals with serious mental illnesses and reduce their overrepresentation in the criminal justice system. A summary of these practices is provided in Figure 1. These include mental health training for law enforcement and correctional officers, mental health court diversion programs, mental health screening in custody, comprehensive transitional planning, community supervision, and community-based mental health services. A prominent theme of this review, however, is the lack of resources to carry out these activities. In order to effectively manage criminal justice-involved people with SMIs and reduce their overrepresentation in the criminal justice system, more resources would need to be allocated to mental health services, particularly in the community. Increasing resources to address mental health needs in the community has the potential of preventing and reducing criminal justice system involvement among individuals with SMIs. Addressing the needs of people with SMIs in the community is also more cost effective than incarceration. Finally, it is essential that we conduct more rigorous evaluations of approaches designed to address the needs of individuals with SMIs in Canada.
Figure 1. Promising practices for addressing the needs of criminal justice-involved individuals with serious mental illnesses
References
Al-Rousan, T., Rubenstein, L., Sieleni, B., Deol, H., & Wallace, R. (2017). Inside the nation’s largest mental health institution: A prevalence study in a state prison system. BMC Public Health, 17(1), 342-351. https://doi.org/10.1186/s12889-017-4257-0
Andrews, D. A., Bonta, J., & Hoge, R. D. (1990). Classification for effective rehabilitation: Rediscovering psychology. Criminal Justice and Behavior, 17(1), 19-52. https://doi.org/10.1177/0093854890017001004
Anestis, J. C., & Carbonell, J. L. (2014). Stopping the revolving door: Effectiveness of mental health court in reducing recidivism by mentally ill offenders. Psychiatric Services, 65(9), 1105-1112. https://doi.org/10.1176/appi.ps.201300305
Appelbaum, K. L., Hickey, J. M., & Packer, I. (2001). The role of correctional officers in multidisciplinary mental health care in prisons. Psychiatric Services, 52(10), 1343-1347. https://doi.org/10.1176/appi.ps.52.10.1343
Barnao, M., & Ward, T. (2015). Sailing uncharted seas without a compass: A review of interventions in forensic mental health. Aggression and Violent Behavior, 22, 77-86. https://doi.org/10.1016/j.avb.2015.04.009
BC Mental Health and Substance Use Services. (2017). Overview of PHSA correctional health services. http://www.bcmhsus.ca/Documents/CHS_Overview-09-29-Final.pdf
BC Mental Health and Substance Use Services. (2019). Correctional health services: About. http://www.bcmhsus.ca/our-services/health-services-for-people-in-custody/correctional-health-services
Beaudette, J. N., Power, J., & Stewart, L. A. (2015). National prevalence of mental disorders among incoming federally-sentenced men offenders. Correctional Service Canada. https://www.csc-scc.gc.ca/research/005008-0357-eng.shtml
Beaudette, J. N., & Stewart, L. A. (2016). National prevalence of mental disorders among incoming Canadian male offenders. The Canadian Journal of Psychiatry/La Revue Canadienne de Psychiatrie, 61(10), 624-632. https://doi.org/10.1177/0706743716639929
Bill C-83 An Act to amend the Corrections and Conditional Release Act and another Act. (2019). Royal Assent June 21st, 2019, 42nd Parliament, 1st Session. Parliament of Canada. https://www.parl.ca/LegisInfo/BillDetails.aspx?Language=E&billId=10078426
Bland, R. C., Newman, S. C., Thompson, A. H., & Dyck, R. J. (1998). Psychiatric disorders in the population and in prisoners. International Journal of Law and Psychiatry.21(3), 273-279. https://doi.org/10.1016/S0160-2527(98)00005-3
Bonfine, N., Wilson, A. B., & Munetz, M. R. (2020). Meeting the needs of justice-involved people with serious mental illness within community behavioral health systems. Psychiatric Services, 71(4), 355-363. https://doi.org/10.1176/appi.ps.201900453
Bonta, J., & Andrews, D. A. (2017). The psychology of criminal conduct (6th ed.). Routledge.
Bonta, J., Blais, J., & Wilson, H. A. (2014). A theoretically informed meta-analysis of the risk for general and violent recidivism for mentally disordered offenders. Aggression and Violent Behavior, 19(3), 278-287. https://doi.org/10.1016/j.avb.2014.04.014
Bonta, J., Bourgon, G., Rugge, T., Pedneault, C., & Lee, S. C. (in press). A system-wide implementation and evaluation of the Strategic Training Initiative in Community Supervision (STICS). Public Safety Canada.
Bonta, J., Bourgon, G., Rugge, T., Scott, T. L., Yessine, A. K., Gutierrez, L., & Li, J. (2011). An experimental demonstration of training probation officers in evidence-based community supervision. Criminal Justice and Behavior, 38(11), 1127-1148. https://doi.org/10.1177/0 093854811420678
Bonta, J., Law, M., & Hanson, K. (1998). The prediction of criminal and violent recidivism among mentally disordered offenders: A meta-analysis. Psychological Bulletin, 123(2), 123-142. https://doi.org/10.1037/0033-2909.123.2.123
Brink, J. H., Doherty, D., & Boer, A. (2001). Mental disorder in federal offenders: A Canadian prevalence study. International Journal of Law and Psychiatry, 24(4-5), 339-356. https://doi.org/10.1016/S0160-2527(01)00071-1
Brown, G.P., Barker, J., McMillan, K., Norman, R., Derkzen, D., Stewart, L.A., & Wardrop, K. (2018). Prevalence of mental disorder among federal women offenders: Intake and in-custody. Correctional Service Canada. https://www.csc-scc.gc.ca/research/r-40-en.shtml
Brown, G. P., Hirdes, J. P., & Fries, B. E. (2015). Measuring the prevalence of current, severe symptoms of mental health problems in a Canadian correctional population: Implications for delivery of mental health services for inmates. International Journal of Offender Therapy and Comparative Criminology, 59(1), 27-50. https://doi.org/10.1177/0306624 X13507040
Canada, Parliament, Senate. Standing Senate Committee on Human Rights. (2019). Interim report – study on the human rights of federally-sentenced persons: The most basic human right is to be treated as a human being (1 February 2017-26 March 2018). https://sencanada.ca/content/sen/committee/421/RIDR/Reports/RIDR_Report_Prisioners_e.pdf
Canadian Centre on Substance abuse. (2009). Substance abuse in Canada: Concurrent disorders. https://ccsa.ca/sites/default/files/2019-04/ccsa-011811-2010.pdf
Canadian Public Health Association (2004). A health care needs assessment of federal inmates in Canada. Canadian Journal of Public Health. 95(1), S1-S63. https://www.jstor.org/stable/ 41994314
Chang, Z., Lichtenstein, P., Långström, N., Larsson, H., & Fazel, S. (2016). Association between prescription of major psychotropic medications and violent reoffending after prison release. JAMA, 316(17), 1798-1807. https://doi.org/10.1001/jama.2016.15380
Charette, Y., Crocker, A. G., & Billette, I. (2014). Police encounters involving citizens with mental illness: Use of resources and outcomes. Psychiatric Services, 65(4), 511-516. https://doi.org/10.1176/appi.ps.201300053
COAST Hamilton (n.d.). COAST services. https://coasthamilton.ca/?page_id=57
Coleman, T. & Cotton, D. (2014). TEMPO: Police interactions – A report towards improving interactions between police and people living with mental health problems. Mental Health Commission of Canada. https://www.mentalhealthcommission.ca/sites/default/ files/2016-05/TEMPO%20Police%20Interactions%20082014.pdf
ConnexOntario. (2019). Pre-charge diversion. https://www.connexontario.ca/Directory/Program/ 12282
Constantine, R. J., Robst, J., Andel, R., & Teague, G. (2012). The impact of mental health services on arrests of offenders with a serious mental illness. Law and Human Behavior, 36(3), 170-176. https://doi.org/10.1037/h0093952
Corrado, R. R., Cohen, I., Hart, S., & Roesch, R. (2000). Comparative examination of the prevalence of mental disorders among jailed inmates in Canada and the United States. International Journal of Law and Psychiatry, 23(5-6), 633-647. https://doi.org/10.1016/S0160-2527(00)00054-6
Correctional Service Canada. (2009). The changing federal offender population: Highlights 2009. https://www.csc-scc.gc.ca/research/sr-2009-eng.shtml
Correctional Service Canada. (2012a). Mental health strategy for corrections in Canada. http://publications.gc.ca/collections/collection_2013/scc-csc/PS84-26-2012-eng.pdf
Correctional Service Canada. (2012b). Towards a continuum of care: Correctional Service Canada mental health strategy. https://www.csc-scc.gc.ca/health/002006-2000-eng.shtml
Correctional Service Canada. (2013). Coroner’s inquest touching the death of Ashley Smith. https://www.csc-scc.gc.ca/publications/005007-9009-eng.shtml
Correctional Service Canada. (2018). Computerized mental health intake screening system. Technical manual version 2.4 [Unpublished report].
Cotton, D. H., & Coleman, T. G. (2008, November). A study of police academy training and education for new police officers related to working with people with mental illness. Mental Health Commission of Canada and the Canadian Association of Chiefs of Police. https://www.mentalhealthcommission.ca/sites/default/files/Law_Police_Academy_Training_Education_Mental_Illness_Study_ENG_0_1.pdf
Criminal Code, R.S.C., (1985), c. C-46
Crocker, A. G., Nicholls, T. L., Seto, M. C., Côté, G., Charette, Y., & Caulet, M. (2015). The National Trajectory Project of individuals found not criminally responsible on account of mental disorder in Canada. Part 1: Context and methods. The Canadian Journal of Psychiatry, 60(3), 98-105. https://doi.org/10.1177/070674371506000304
Cusack, K. J., Morrissey, J. P., Cuddeback, G. S., Prins, A., & Williams, D. M. (2010). Criminal justice involvement, behavioral health service use, and costs of forensic assertive community treatment: A randomized trial. Community Mental Health Journal, 46(4), 356-363. https://doi.org/10.1007/s10597-010-9299-z
Delveaux, K., MacDonald, C., McConnell, A., Bradley, S., Crawford, A., & Tse, F. (2017). Evaluation of CSC’s health services. Correctional Service Canada. https://www.csc-scc.gc.ca/publications/092/005007-2017-eng.pdf
Derkzen, D., Booth, L., Taylor, K., & McConnell, A. (2013). Mental health needs of federal female offenders. Psychological Services, 10(1), 24-36. https://doi.org/10.1037/a0029653
Derogatis, L. R. (1993). BSI, Brief Symptom Inventory. Administration, scoring, and procedures manual (4th ed.). National Computer Systems.
Desai, A. (2010). Community connections: The key to community corrections for individuals with mental health disorders. St. Leonard’s Society of Canada. http://www.stleonards.ca/wp-content/uploads/2013/05/Community-Connections-The-Key-to-Community-Corrections-for-Individuals-with-Mental-Health-Disorders-20101.pdf
Desai, A., Delisle, C., Lewchuk, J., & Wilson, J. D. (2013). Towards an integrated network: Working together to avoid criminalization of people with mental health problems. St. Leonard’s Society of Canada. http://www.stleonards.ca/wpcontent/uploads/2013/05/To wards-an-Integrated-Network-Working-Together-to-Avoid-Criminalization-of-People-with-Mental-Health-Problems-2008.pdf
Deslich, S. A., Thistlethwaite, T., & Coustasse, A. (2013). Telepsychiatry in correctional facilities: Using technology to improve access and decrease costs of mental health care in underserved populations. The Permanente Journal, 17(3), 80-86. https://doi.org/10.7812/ TPP/12-123
Durbin, J., Lin, E., & Zaslavska, N. (2010). Police-citizen encounters that involve mental health concerns: Results of an Ontario police services survey. Canadian Journal of Community Mental Health, 29(S5), 53-7. https://doi.org/10.7870/cjcmh-2010-0034
Epperson, M. W., Wolff, N., Morgan, R. D., Fisher, W. H., Frueh, B. C., & Huening, J. (2014). Envisioning the next generation of behavioral health and criminal justice interventions. International Journal of Law and Psychiatry, 37(5), 427-438. https://doi.org/10.1016/j.ijlp.2014.02.015
Farrell MacDonald, S., Keown, L. A., Boudreau, H., Gobeil, R., & Wardrop, K. (2015). Prevalence of psychotropic medication prescription among federal offenders. Correctional Service Canada. http://publications.gc.ca/collections/collection_2017/scc-csc/PS83-3-373-eng.pdf
Farrell MacDonald, S., Stewart, L. A., & Feeley, S. (2014). The impact of the Community Mental Health Initiative (CMHI). Correctional Service Canada. https://www.csc-scc.gc.ca/research/005008-0337-eng.shtml
Fazel, S., Hayes, A. J., Bartellas, K., Clerici, M., & Trestman, R. (2016). Mental health of prisoners: Prevalence, adverse outcomes, and interventions. The Lancet Psychiatry, 3(9), 871-881. https://doi.org/10.1016/S2215-0366(16)30142-0
Fazel, S., & Seewald, K. (2012). Severe mental illness in 33,588 prisoners worldwide: systematic review and meta-regression analysis. The British Journal of Psychiatry, 200(5), 364–373. https://doi.org/10.1192/bjp.bp.111.096370
Ferrazzi, P., & Krupa, T. (2018). Remoteness and its impact on the potential for mental health initiatives in criminal courts in Nunavut, Canada. International Journal of Circumpolar Health, 77(1), 154700. https://doi.org/10.1080/22423982.2018.1541700
Fontanarosa, J., Uhl, S., Oyesanmi, O., & Schoelles, K. M. (2013). Interventions for adult offenders with serious mental illness. Agency for Healthcare Research and Quality. https://effectivehealthcare.ahrq.gov/sites/default/files/pdf/mental-ill ness-adults-prisons_research.pdf
Hoch, J. & Hartford, K. & Heslop, L. & Stitt, L. (2009). Mental illness and police interactions in a mid-sized Canadian city: What the data do and do not say. Canadian Journal of Community Mental Health. 28(1), 49-66. https://doi.org/10.7870/cjcmh-2009-0005
Hoffman, R., Hirdes, J., Brown, G. P., Dubin, J. A., & Barbaree, H. (2016). The use of a brief mental health screener to enhance the ability of police officers to identify persons with serious mental disorders. International Journal of Law and Psychiatry, 47, 28-35. https://doi.org/10.1016/j.ijlp.2016.02.031
Honegger, L. N. (2015). Does the evidence support the case for mental health courts? A review of the literature. Law and Human Behavior, 39(5), 478-488. https://doi.org/10.1037/lhb0000 141
Human Services and Justice Coordinating Committee. (1997). A provincial strategy to coordinate human services and CJSs in Ontario. http://hsjcc.on.ca/wp-content/uploads/Provincial-Strategy-to-Coordinate-Human-Services-and-Criminal-Justice-Systems-1997.pdf
IACFP Practice Standards Committee. (2010). Standards for psychology services in jails, prisons, correctional facilities, and agencies (3rd edition). Criminal Justice and Behavior, 37(7), 749-808. https://doi.org/10.1177/0093854810368253
Jakobowitz, S., Bebbington, P., McKenzie, N., Iveson, R. Duffield, G. Kerr, M. & Killaspy, H. (2017). Assessing needs for psychiatric treatment in prisoners: 2 Met and unmet need. Social Psychiatry and Psychiatric Epidemiology, 52(2), 231-240. https://doi.org/10.10 07/s00127-016-1313-5
Johns, A. (2001). Psychiatric effects of cannabis. British Journal of Psychiatry, 178(2), 116-122. https://doi.org/10.1192/bjp.178.2.116
Koziarski, J. (2018). Policing mental health: An exploratory study of crisis intervention teams and co-response teams in the Canadian context (Publication No. 13804325) [Doctoral dissertation, University of Ontario Institute of Technology]. ProQuest Dissertations Publishing.
Lafortune, D. (2010). Prevalence and screening of mental disorders in short-term correctional facilities. International Journal of Law and Psychiatry, 33(2), 94-100. https://doi.org/1 0.1016/j.ijlp.2009.12.004
Leschied, A. W. (2011). The treatment of incarcerated mentally disordered women offenders: A synthesis of current research. Public Safety Canada. https://www.publicsafety.gc.ca/cnt/r srcs/pblctns/2011-03-tmdw/index-en.aspx
Livingston, J. (2009). Mental health and substance use services in correctional settings: A review of minimum standards and best practices. International Centre for Criminal Law Reform and Criminal Justice. https://icclr.law.ubc.ca/publication/mental-health-and-substance-use-services-in-correctional-settings-a-review-of-minimum-standards-and-best-practices/
Manchak, S. M., Skeem, J. L., Kennealy, P. J., & Louden, J. E. (2014). High-fidelity specialty mental health probation improves officer practices, treatment access, and rule compliance. Law and Human Behavior, 38(5), 450-461. https://doi.org/10.1037/lhb0000 076
Mann, B., Bond, D., & Powitzky, R. J. (2011). Collaborating for SUCCESS in interagency correctional mental health reentry. Corrections Today, 73(5), 30–33. http://doc.ok.gov/ collaborating-for-success-in-interagency-correctional-mental-health-reentry
Martin, M. S., Colman, I., Simpson, A. I., & McKenzie, K. (2013a). Mental health screening tools in correctional institutions: A systematic review. BMC Psychiatry, 13(1). https://bmcpsychiatry.biomedcentral.com/articles/10.1186/1471-244X-13-275
Martin, M. S., Colman, I., Simpson, A. I., & McKenzie, K. (2013b). Mental health screening tools in correctional institutions: A systematic review [Additional File 1]. BMC Psychiatry, 13(1). https://bmcpsychiatry.biomedcentral.com/articles/10.1186/1471-244X-13-275
Martin, M. S., Crocker, A. G., Potter, B. K., Wells, G. A., Grace, R. M., & Colman, I. (2018). Mental health screening and differences in access to care among prisoners. The Canadian Journal of Psychiatry, 63(10), 692-700. https://doi.org/0706743718762099.
Martin, M. S., Potter, B. K., Crocker, A. G., Wells, G. A., Grace, R. M., & Colman, I. (2018). Mental health treatment patterns following screening at intake to prison. Journal of Consulting and Clinical Psychology, 86(1), 15-23. https://doi.org/10.1037/ccp0000259
Martin, M.S., Wamboldt, A. D., O’connor, S. L., Fortier, J., & Simpson, A. I. (2013). A comparison of scoring models for computerised mental health screening for federal prison inmates. Criminal Behaviour and Mental Health, 23(1), 6-17. https://doi.org/10.10 02/cbm.1853
Martin, M. S., Wells, G. A., Crocker, A. G., Potter, B. K., & Colman, I. (2018a). Decision curve analysis as a framework to estimate the potential value of screening or other decision‐making aids. International journal of methods in psychiatric research, 27(1), e1601. http s://doi.org/10.1002/mpr.1601
Martin, M. S., Wells, G. A., Crocker, A. G., Potter, B. K., & Colman, I. (2018b). Mental health screening, treatment, and institutional incidents: A propensity score matched analysis of long-term outcomes of screening. International Journal of Forensic Mental Health, 17(2), 133-144. https://doi.org/10.1080/14999013.2018.1451415
McKee, S. A. (2017). Concurrent substance use disorders and mental illness: Bridging the gap between research and treatment. Canadian Psychology, 58(1), 50-57. https://doi.org/10. 1037/cap0000093
Mental Health Commission of Canada (2012). Changing directions, changing lives: The mental health strategy for Canada. https://www.mentalhealthcommission.ca/sites/default/files/M HStrategy_Strategy_ENG.pdf
Mills, J.F., & Kroner, D.G. (2004). A new instrument to screen for depression, hopelessness and suicide in offenders. Psychological Services, 1(1), 83–91. https://doi.org/10.1037/1541-1559.1.1.83
Morgan, R. D., Flora, D. B., Kroner, D. G., Mills, J. F., Varghese, F., & Steffan, J. S. (2012). Treating offenders with mental illness: A research synthesis. Law and Human Behavior, 36(1), 37-50. https://doi.org/10.1037/h0093964
Morgan, R. D., Steffan, J., Shaw, L. B., & Wilson, S. (2007). Needs for and barriers to correctional mental health services: Inmate perceptions. Psychiatric Services, 58(9), 1181-1186. https://doi.org/10.1176/ps.2007.58.9.1181
National Institute of Mental Health (2017). Borderline personality disorder. Retrieved November 28, 2019, from https://www.nimh.nih.gov/health/topics/borderline-personality-disorder/index.shtml
Nilson, W. (2016). Collaborative risk-driven intervention: A study of Samson Cree Nation’s application of the Hub Model. Public Safety Canada. https://www.publicsafety.gc.ca/cnt/rsrcs/pblctns/2016-r001/index-en.aspx
Office of the Correctional Investigator (2013). Annual report of the Office of the Correctional Investigator 2014-2015. https://www.oci-bec.gc.ca/cnt/rpt/annrpt/annrpt20122013-eng.aspx#sI
Office of the Correctional Investigator (2015). Annual report of the Office of the Correctional Investigator 2014-2015. https://www.oci-bec.gc.ca/cnt/rpt/pdf/annrpt/annrpt20142015-eng.pdf
Ogloff, J. R., Talevski, D., Lemphers, A., Wood, M. & Simmons, M. (2015). Co-occurring mental illness, substance use disorders, and antisocial personality disorders among clients of forensic mental health services. Psychiatric Rehabilitation Journal, 31, 16-23. doi:10.1037/prj0000088
Osher, F., Steadman, H. J., & Barr, H. (2003). A best practice approach to community reentry from jails for inmates with co-occurring disorders: The APIC model. Crime & Delinquency, 49(1), 79-96. https://doi.org/10.1177/0011128702239237
Parekh, R. (2018, August). What is mental illness? American Psychiatric Association. https://www.psychiatry.org/patients-families/what-is-mental-illness
Prins, S. J., & Draper, L. (2009). Improving outcomes for people with mental illnesses under community corrections supervision: A guide to research-informed policy and practice. National Institute of Corrections. https://www.ncjrs.gov/App/AbstractDB/AbstractDBDet ails.aspx?id=249355
Prins, S. J., Osher, F. C., Steadman, H. J., Robbins, P. C., & Case, B. (2012). Exploring racial disparities in the Brief Jail Mental Health Screen. Criminal Justice and Behavior, 39 (5), 635-645. https://doi.org/10.1177/0093854811435776.
Public Safety Canada (2019). Corrections and conditional release statistical overview: 2018 annual report. https://www.publicsafety.gc.ca/cnt/rsrcs/pblctns/ccrso-2018/index-en.aspx
Rezansoff, S. N., Moniruzzaman, A., Fazel, S., McCandless, L., & Somers, J. M. (2017). Adherence to antipsychotic medication and criminal recidivism in a Canadian provincial offender population. Schizophrenia Bulletin, 43(5), 1002-1010. https://doi.org/10.1093/schbul/sbx084
Royal Ottawa Mental Health Care Group. (n.d.). Areas of care: Mental health and the law. http:// www.theroyal.ca/mental-health-centre/mental-health-programs/areas-of-care/mental-health-and-the-law/
Sales, C. P., McSweeney, L., Saleem, Y., & Khalifa, N. (2018). The use of telepsychiatry within forensic practice: A literature review on the use of videolink – a ten-year follow-up. The Journal of Forensic Psychiatry & Psychology, 29(3), 387-402. https://doi.org/10.1080/14 789949.2017.1396487
Sarteschi, C. M., Vaughn, M. G., & Kim, K. (2011). Assessing the effectiveness of mental health courts: A quantitative review. Journal of Criminal Justice, 39(1), 12-20. https://doi.org/10.1016/j.jcrimjus.2010.11.003
Schneider, R. D. (2010). Mental health courts and diversion programs: A global survey. International Journal of Law and Psychiatry, 33(4), 201-206. https://doi.org/10.1016/j.ijlp.2010.07.001
Scott, R. L. (2000). Evaluation of a mobile crisis program: Effectiveness, efficiency, and consumer satisfaction. Psychiatric Services, 51(9), 1153-1156. https://doi.org/10.1176 /appi.ps.51.9.1153
Seto, M. C., Basarke, S., Healey, L. V., & Sirotich, F. (2018). Correlates of mental health diversion completion in a Canadian consortium. International Journal of Forensic Mental Health, 17(1), 1-12. https://doi.org/10.1080/14999013.2017.1405123
Shapiro, G. K., Cusi, A., Kirst, M., O’Campo, P., Nakhost, A., & Stergiopoulos, V. (2015). Co-responding police-mental health programs: A review. Administration and Policy in Mental Health, 42(5), 606-620. https://doi.org/10.1007/s10488-014-0594-9
Simpson, A. I., McMaster, J. J., & Cohen, S. N. (2013). Challenges for Canada in meeting the needs of persons with serious mental illness in prison. Journal of the American Academy of Psychiatry and the Law Online, 41(4), 501-509. https://www.ncbi.nlm.nih.gov/pubmed /24335321
Skeem, J. L., Manchak, S., & Peterson, J. K. (2011). Correctional policy for offenders with mental illness: Creating a new paradigm for recidivism reduction. Law and Human Behavior, 35(2), 110-126. https://doi.org/10.1007/s10979-010-9223-7
Skeem, J. L., Steadman, H. J., & Manchak, S. M. (2015). Applicability of the risk-need-responsivity model to persons with mental illness involved in the CJS. Psychiatric Services, 66(9), 916-922. https://doi.org/10.1176/appi.ps.201400448
Skeem, J. L., Winter, E., Kennealy, P. J., Louden, J. E., & Tatar, J. R., (2014). Offenders with mental illness have criminogenic needs, too: Toward reducing recidivism. Law and Human Behavior, 38(3), 212-224. https://doi.org/10.1037/lhb0000054
Slinger, E., & Roesch, R. (2010). Problem-solving courts in Canada: A review and a call for empirically-based evaluation methods. International Journal of Law and Psychiatry, 33(4), 258-264. https://doi.org/10.1016/j.ijlp.2010.06.008
Statistics Canada (2018). First Nations people, Métis and Inuit in Canada: Diverse and growing populations. https://www150.statcan.gc.ca/n1/pub/89-659-x/89-659-x2018001-eng.htm
Steadman, H. J., Redlich, A., Callahan, L., Robbins, P. C., & Vesselinov, R. (2011). Effect of mental health courts on arrests and jail days: A multisite study. Archives of General Psychiatry, 68(2), 167-172. https://doi.org/10.1001/archgenpsychiatry.2010.134
Stewart, L. A., Gamwell, L., & Wilton, G. (2018). Comorbid mental disorders: Prevalence and impact on community outcomes. Correctional Service Canada. https://www.csc-scc.gc.ca/research/r-404-en.shtml
Stewart, L. A., & Wilton, G. (2017). Comorbid mental disorders: Prevalence and impact on institutional outcomes. Correctional Service Canada. https://www.csc-scc.gc.ca/research/r-379-en.shtml
Swofford, C. D., Kasckow, J. W., Scheller-Gilkey, G., & Inderbitzin, L. B. (1996). Substance use: A powerful predictor of relapse in schizophrenia. Schizophrenia Research, 20(1-2), 145-151. https://doi.org/10.1016/0920-9964(95)00068-2
Watts, J., & Weinrath, M. (2017). The Winnipeg Mental Health Court: Preliminary findings on program implementation and criminal justice outcomes. Canadian Journal of Community Mental Health, 36(1), 67-82. https://doi.org/10.7870/cjcmh-2017-005
Yoon, I. A., Slade, K., & Fazel, S. (2017). Outcomes of psychological therapies for prisoners with mental health problems: A systematic review and meta-analysis. Journal of Consulting and Clinical Psychology, 85(8), 783-802. https://doi.org/10.1s37/ccp0000
Appendix: Non-Pharmaceutical Treatment Approaches for Criminal Justice-Involved Individuals with Serious Mental Illness
| Approach | Description | Types/Features | Strengths | Weaknesses | References |
| Assertive Community Treatment |
|
|
|
|
|
| Behavioural Therapy |
|
|
|
|
|
| Changing Lives and Changing Outcomes (CLCO) |
|
|
|
|
|
| Cognitive Behavioural Therapy |
|
|
|
|
|
| Dialectic Behavioural Therapy (correctional adaptation) |
|
|
|
|
|
| Reasoning and Rehabilitation (R&R) |
|
|
|
|
|
| Reasoning and Rehabilitation 2: Mental Health Program (R&RMHP) |
|
|
|
|
|
| Therapeutic Community |
|
|
|
|
|
Note. Treatment approaches are listed in alphabetical order and not based on effectiveness. CJI-MI = criminal justice-involved individuals with mental illnesses.
References for Appendix table
Blanchette, K., Flight, J., Verbrugge, P., Gobeil, R., & Taylor, K. (2011). Dialectical behaviour therapy within a women’s structured living environment. Correctional Service Canada. https://www.csc-scc-gc.ca/research/005008-0241-eng.shtml
Cullen, A., Clarke, A., Kuipers, E., Hodgins, S., Dean, K., Fahy, T. (2012). A multisite randomized trial of a cognitive skills programme for male mentally disordered offenders: Social-cognitive outcomes. Psychological Medicine, 42(3), 557–569. https://doi.org/10.1017/S0033291711001553
C-Y Yip, V., Gudjonsson, G. H., Perkins, D., Doidge, A., Hopkin, G., Young, S. (2013). A non-randomised controlled trial of the R&R2MHP cognitive skills program in high risk male offenders with severe mental illness. BMC Psychiatry, 13(1), 267-278. https://doi.org/10.1186/1471-244X-13-267
Eljdupovic, E., Lapierre, D., & Reimer, J. (2016). Dialectics associated with implementation of Dialectical Behaviour Therapy in Canadian federal correctional institutions for women. Suicidiologi, 21(2), 16-23. https://doi.org/10.5617/suicidologi.3887
Galassi, A., Mpofu, E., & Athanasou, J. (2015). Therapeutic community treatment of an inmate population with substance use disorders: Post-release trends in re-arrest, re-incarceration, and drug misuse relapse. International Journal of Environmental Research and Public Health, 12(6), 7059-7072. https://doi.org/10.3390/ijerph120607059
Knabb, J. J., Welsh, R. K., & Graham-Howard, M. L. (2011). Treatment alternatives for mentally disordered offenders: A review of the literature. Psychology, 2(2), 122-131. https://doi.or g/10.4236/psych.2011.22020
Lamberti, J., Weisman, R., & Faden, D. (2004). Forensic assertive community treatment: Preventing incarceration of adults with severe mental illness. Psychiatric Services, 55(11), 1285-1293. https://doi.org/10.1176/appi.ps.55.11.1285
McDonagh, D., Taylor, K., & Blanchette, K. (2015). Correctional adaptation of Dialectic Behaviour Therapy (DBT) for federally sentenced women. Forums on Corrections Research, 14(2), 36-39. https://www.csc-scc.gc.ca/research/forum/e142/e142i-eng.shtml
McKendrick, K., Sullivan, C., Banks, S., & Sacks, S. (2006). Modified therapeutic community treatment for offenders with mica disorders: Antisocial personality disorder and treatment outcomes. Journal of Offender Rehabilitation, 44(2-3), 133-159. https://doi.org/10.1300/J 076v44n02_06
Morgan, R. D., Kroner, D. G., Mills, J. F., Bauer, R. L., & Serna, C. (2014). Treating justice involved persons with mental illness: Preliminary evaluation of a comprehensive treatment program. Criminal Justice and Behavior, 41(7), 902-916. https://doi.org/10.11 77/0093854813508553
Rampling, J., Furtado, V., Winsper, C., Marwaha, S., Lucca, G., Livanou, M., & Singh, S. P. (2016). Non-pharmacological interventions for reducing aggression and violence in serious mental illness: A systematic review and narrative synthesis. European Psychiatry, 34, 17-28. https://doi.org/10.1016/j.eurpsy.2016.01.2422
Van Horn, S. A., Morgan, R. D., Brusman-Lovins, L., Littlefield, A. K., Hunter, J. T., Gigax, G., & Ridley, K. (2018). Changing lives and changing outcomes: “What works” in an intervention for justice-involved persons with mental illness. Psychological Services, 16(4), 693-700. https://doi.org/10.1037/ser0000248
Footnotes
- 1“Borderline personality disorder is an illness marked by an ongoing pattern of varying moods, self-image, and behavior. These symptoms often result in impulsive actions and problems in relationships. People with borderline personality disorder may experience intense episodes of anger, depression, and anxiety that can last from a few hours to days” (The National Institute of Mental Health, 2017, Para 1).
- 2Medication possession ratio “represents the percentage of time that an individual was dispensed prescribed medication (i.e., the number of days of medication supplied within a refill interval divided by the total number of days in the interval)” (Rezansoff et al., 2017, pp. 1003).
- 3An open admission policy allows new individuals to join the therapy group throughout the program; whereas, a closed admission policy only allows individuals to enter the group at the beginning of the treatment program (Morgan et al., 2012).
- 4These inmates received treatment for more than 10% of the time they were incarcerated (Martin, Potter et al., 2018).
IHT5






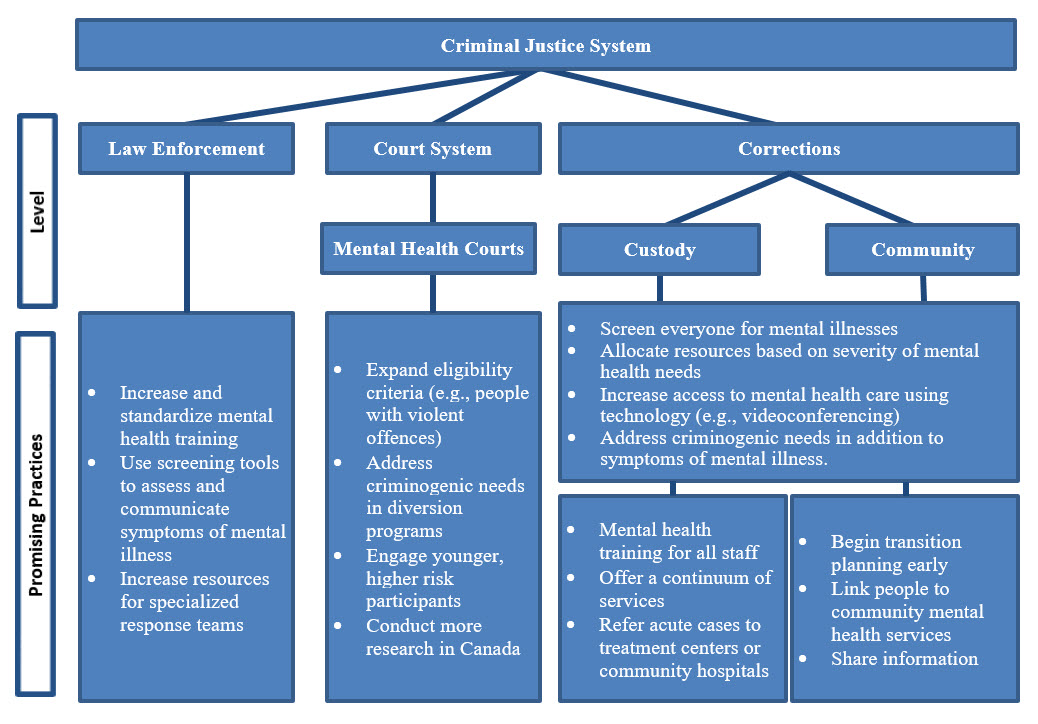{kind=link}